← Back to Course
Thompson Health · Nursing Education
Dysrhythmia
Recognition & Response
Student Follow-Along Coursebook
Class Edition · 2026
F.F. Thompson Hospital · Canandaigua, NY
For educational use during class presentation
Follow along as your instructor covers each topic
Table of Contents
Dysrhythmia Recognition & Response · 2026
This workbook follows the live class presentation. Fill in blanks during lecture.
Use the notes spaces to capture what your instructor emphasizes.
| Modules |
| 1 · Introduction & Conduction System | 3 |
| 2 · AV Blocks (Heart Blocks) | 4–5 |
| 3 · Pacemakers | 6 |
| 4 · ECG Basics & The 5-Step Method | 7–9 |
| 5 · Sinus Rhythms | 10 |
| 6 · Atrial Rhythms (PAC / Flutter / AFib / SVT) | 11 |
| 7 · Junctional Rhythms | 12 |
| 8 · Ventricular Rhythms & Arrest | 13 |
| Reference Tools |
| Rhythm Identification Flowchart | 14 |
| Practice |
| Practice Strips (20 strips — unlabeled) | 15–24 |
| Final Assessment — Capstone Strips | 25 |
How to use this booklet: Your instructor will present each module using the course slides.
As they teach, fill in the blanks in each section. The blanks are clues — they mark the most important facts to remember.
Each module includes a practice strip — apply what you just learned before moving on.
Why AV Blocks & Pacemakers Come First: Understanding why conduction can fail — and how we compensate — makes every subsequent rhythm click into place.
Learn the blocks, then the 5-step method will feel like second nature.
The Clinical Mantra
Recognize → Assess → Act.
Every rhythm you learn leads to a clinical decision. Rate and rhythm on paper only matter in the context of how your patient looks.
2
Module 1 · Introduction & Conduction System
Foundation
The Clinical Approach
- The three-step mantra: Recognize → Assess → Act
- Always treat the patient, not the monitor
- Signs of instability: hypotension, chest pain, dyspnea / shortness of breath, altered level of consciousness
The Electrical Pathway
Fill in the conduction pathway in order:
SA Node
→
AV Node
→
Bundle of His
→
Bundle Branches
→
Purkinje Fibers
Pacemaker Hierarchy
| Pacemaker Site |
Intrinsic Rate |
Resulting Rhythm If Primary |
| SA Node |
60 – 100 bpm |
Normal Sinus Rhythm |
| AV Junction |
40 – 60 bpm |
Junctional rhythm |
| Ventricles |
20 – 40 bpm |
Idioventricular rhythm |
Key Point
Higher pacemakers suppress lower ones. If the SA node fails, the AV junction takes over — but at a slower rate.
Each backup pacemaker is a safety net, not a normal state.
3
Module 2 · AV Blocks (Heart Blocks)
Rhythm Recognition · AV Node
All AV blocks share one feature: delayed or impaired conduction between atria and ventricles.
| Block Type |
PR Interval |
Dropped Beats? |
QRS |
Risk Level |
| 1st Degree |
> 0.20 sec, constant |
None |
Narrow |
Low — benign |
| 2nd Degree Type I (Wenckebach) |
Progressively lengthens |
Yes — periodically |
Usually narrow |
Low–moderate |
| 2nd Degree Type II (Mobitz II) |
Normal/constant (fixed) |
Yes — suddenly |
Often wide |
High — can progress to 3rd degree |
| 3rd Degree (Complete) |
Variable/absent (no relationship) |
Complete dissociation |
Wide (ventricular) or narrow (junctional) |
Critical — emergent pacing |
♥ Heart Block Decision Tree
START: Look at the PR intervals — are they consistent?
↓
BRANCH A — PR is FIXED (same before every beat)
Are ALL beats conducted? (No dropped QRS?)
YES ↓
PR > 0.20 sec?
YES ↓
✔ First-Degree AV Block
PR prolonged but constant; all beats conduct
NO ↓
Normal conduction
Not a block — PR is normal & all beats present
NO — beats are dropped ↓
QRS drops suddenly with no warning? (PR fixed right up to the drop)
YES ↓
⚠ Second-Degree Type II — Mobitz II
Fixed PR → sudden QRS disappears. HIGH RISK — can deteriorate to 3rd degree. Prepare to pace.
BRANCH B — PR is VARIABLE (changes beat to beat)
Does the PR progressively lengthen, then a beat drops — then cycle repeats?
YES ↓
↗ Second-Degree Type I — Wenckebach
PR gradually ↑ → dropped QRS → reset → repeat. Usually benign, but monitor.
Are P waves and QRS complexes completely independent? (Different rates, no relationship, no pattern)
↓
🚨 Third-Degree (Complete) Heart Block
AV dissociation. Atria and ventricles march independently. EMERGENT PACING REQUIRED.
⚠ Remember: 3rd degree HAS visible P waves — they just march independently and bear no relationship to the QRS. Do not mistake P waves for "normal conduction."
4
Module 2 (cont.) · AV Blocks — Clinical Details & Practice
Rhythm Recognition · AV Node
Wenckebach (Type I) Clues
- PR gets longer (progressively lengthens) then drops a beat
- Cycle then resets
- The RR intervals get progressively shorter
- Location: usually at AV node
- Generally benign (benign / dangerous)
▶ Strip: Identify — Wenckebach or other?
▶ Strip: Is the PR interval prolonged?
Mobitz II Clues
- PR interval is constant/fixed until a beat drops
- No warning — the QRS just disappears
- Location: below the AV node (Bundle of His)
- Can deteriorate to complete (3rd degree) heart block
- Action: prepare for pacing
▶ Strip: Fixed PR or lengthening?
▶ Strip: Are P waves and QRS related?
Key Point — 3rd Degree Block
Complete AV dissociation: P waves and QRS complexes march on independently.
The atrial rate is faster than the ventricular rate.
This is a medical emergency — the ventricles are running on their own escape rhythm.
5
Module 3 · Pacemakers
Paced Rhythms & Malfunctions
Recognizing Paced Rhythms
- A pacemaker spike appears as a sharp vertical mark
- Atrial pacing: spike before P wave
- Ventricular pacing: spike before QRS (wide QRS)
- Dual-chamber: 2 spikes per beat
- A paced QRS is wide (narrow / wide)
Types of Pacemakers
- Transcutaneous: external, non-invasive, used in emergencies (temporary, external)
- Transvenous: temporary, inserted via central vein
- Permanent: implanted, subcutaneous generator
- VVI mode: paces V, senses V, inhibits on demand
▶ Strip: Find the pacer spikes
Pacemaker Malfunctions
Failure to Capture:
Spike present but no QRS (myocardial response) follows
Causes: lead displacement, increased threshold / exit block, threshold change
Action: increase output / reposition lead
Failure to Sense:
Pacemaker fires despite / on top of a native beat (can't "see" it)
Appears as: spikes in inappropriate places
Risk: R-on-T → ventricular fibrillation
Failure to Pace:
No spike when one is expected
Causes: battery depletion, lead fracture/displacement
Action: troubleshoot pacemaker; apply transcutaneous backup
▶ Strip: Capture present?
▶ Strip: Any sensing issues?
Key Point
Capture = spike followed by a P wave or QRS complex.
If you see a pacemaker spike without a following deflection → failure to capture.
Always assess the patient — is the underlying rate adequate without pacemaker support?
6
Independent Practice — Break 1
Heart Blocks & Pacing · Complete independently · Review with class after break
Interpret each strip using your clinical observation skills. Tip: We'll introduce a systematic 5-step approach in Module 4 — you'll use it for all future strips.
B1-1
Independent Practice — Break 1 (cont.)
Heart Blocks & Pacing · Strips 4–6
B1-2
Independent Practice — Break 1 · Clinical Scenario
Apply: Recognize → Assess → Act
72-year-old male admitted for syncope. History: dual-chamber pacemaker implanted 2 years ago for complete heart block. Current vitals: HR 32, BP 88/52, SpO₂ 94% RA, confused and diaphoretic.
- What rhythm is shown? _______________________________________________
- What is the rate? ___________________________________________________
- Is this patient stable or unstable based on HR 32, BP 88/52, and confusion? _________________________________________
- What is your FIRST nursing action? _________________________________________
B1-3
Module 4 · ECG Basics & Paper Reading
Foundation
ECG Paper — Horizontal (Time)
- 1 small box = 0.04 seconds
- 1 large box = 0.20 seconds
- 5 large boxes = 1 second(s)
- Standard paper speed = 25 mm/sec
ECG Paper — Vertical (Amplitude)
- 1 small box = 0.1 mV
- 1 large box = 0.5 mV
- Standard: 10 mm = 1 mV
Normal Intervals
| Interval | Normal Range |
|---|
| P wave | < 0.12 sec |
| PR interval | 0.12 – 0.20 sec |
| QRS complex | < 0.12 sec |
| QT interval | < 0.44 sec (HR dependent) |
PR in small boxes: 3 to 5 boxes
QRS in small boxes: < 3 boxes
Waveform Meanings
| Waveform / Interval |
Electrical Event |
What it means clinically |
| P wave |
Atrial depolarization |
Atria contract |
| QRS complex |
Ventricular depolarization |
Ventricles contract |
| T wave |
Ventricular repolarization |
Ventricles reset |
| PR interval |
Atrial depolarization + AV node delay |
AV node conduction time |
Key Point
Normal PR = 0.12–0.20 sec (3–5 small boxes). Normal QRS < 0.12 sec (< 3 small boxes).
Wide QRS means the signal traveled an abnormal path through the ventricles.
Now that you've seen what blocks look like — a prolonged PR takes on new meaning!
7
Module 4 (cont.) · The 5-Step Rhythm Method
Core Skill
Apply these steps in order for every rhythm strip. Write the step name in each blank.
1
Step 1: Rhythm
Is the rhythm regular or irregular?
Method: march out RR intervals (caliper or pen method)
2
Step 2: Rate
Count QRS complexes in 6-second strip × 10
Or: 300 ÷ large boxes between beats
3
Step 3: P Waves
Are they present? Y/N
Upright? Y/N
One per QRS? Y/N
4
Step 4: PR Interval
Normal range: 0.12–0.20 sec
Consistent or changing? note if constant, lengthening, or absent
5
Step 5: QRS Width
Normal QRS is narrow (narrow / wide)
Wide QRS suggests: ventricular origin, bundle branch block, or aberrant conduction
Rate Calculation — 6-Second Method
- Count the number of QRS complexes in a 6-second strip
- Multiply by 10 to get beats per minute
- 6 seconds = 30 large boxes on standard ECG paper
- This method works best for irregular rhythms
Key Point
Use the same 5 steps on every strip, every time. Consistency prevents errors.
After every interpretation: "Is this patient stable?"
Quick reminder: Rhythm → Rate → P Waves → PR Interval → QRS Width → Interpret → Act
8
Module 4 (cont.) · Practice: Measurements & The 5-Step Method
Hands-On Practice
Practice: Reading Measurements
Use the ECG intervals diagram below. Find each feature and record your measurements.
- 1. Find a P wave — count small boxes: ~2 boxes = 0.08 sec
- 2. PR interval (start of P → start of QRS): ~4 boxes = 0.16 sec
- 3. QRS width (small boxes): ~2 boxes = 0.08 sec
- 4. Is the PR interval normal? (Normal = 3–5 boxes / 0.12–0.20 sec): Yes — normal
Quick Reference
P wave: < 0.12 sec (< 3 small boxes)
PR interval: 0.12–0.20 sec (3–5 boxes)
QRS: < 0.12 sec (< 3 boxes)
QT: < 0.44 sec (varies with HR)
Practice — Apply the 5 Steps
Use this strip. Walk through all 5 steps out loud before writing your interpretation.
▶ Apply the 5-Step Method — identify this rhythm
Step 1 — Rhythm (regular or irregular?)
Step 2 — Rate (6-sec method)
Step 3 — P Waves (present? upright? 1 per QRS?)
Step 4 — PR Interval (normal / long / variable?)
Step 5 — QRS Width (narrow or wide?)
9
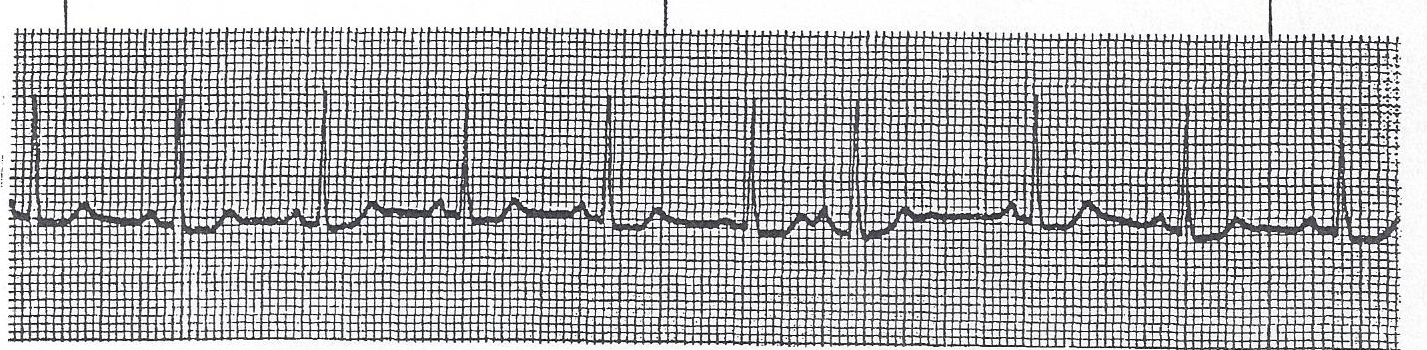
Module 5 · Sinus Rhythms
Rhythm Recognition
| Rhythm |
Rate |
P Waves |
PR / QRS |
Common Cause / Action |
| Normal Sinus Rhythm |
60–100 bpm |
Upright, 1 per QRS |
Normal |
No action needed |
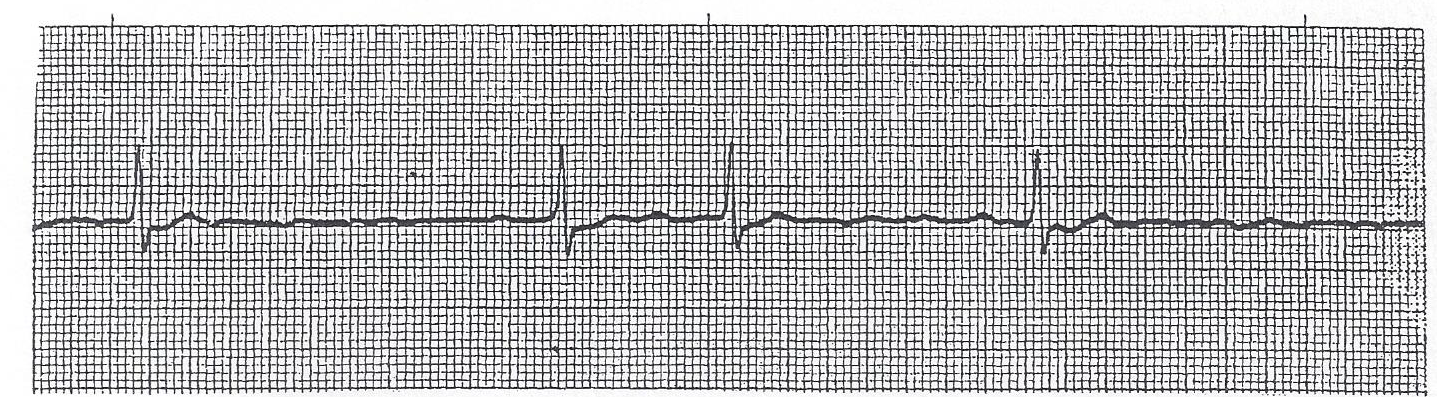
| Sinus Bradycardia |
< 60 bpm |
Normal |
Normal |
Treat if symptomatic |
| Sinus Tachycardia |
> 100 bpm |
Normal |
Normal |
Treat the underlying cause |
| Sinus Arrhythmia |
60–100 bpm |
Normal |
Normal |
Rate varies with respiration |
Key Teaching Points
- All sinus rhythms originate in the SA (sinoatrial) node
- Sinus bradycardia causes: increased vagal tone, hypothyroidism, medications, athletes
- Sinus tachycardia causes: pain, fever, anxiety, hypovolemia, sepsis — always find the cause
- Sinus tachycardia with hemodynamic instability: consider fluid resuscitation; treat underlying cause
- A wandering pacemaker has ≥ 3 different P-wave morphologies
Key Point — Sinus Brady
A rate below 60 bpm is only an emergency if the patient is symptomatic.
Athletes and sleeping patients may have heart rates in the 40s — this is normal for them.
Key Point — Sinus Tachy
Sinus tachycardia is always a response to something (pain, fever, fear, hypovolemia).
Treat the cause, not the number on the monitor.
▶ Practice: Sinus rhythm — fast, slow, or normal?
Step 5 — QRS / Interpretation
Clinical Scenario — Practice
Patient: HR 48 · BP 108/68 · SpO₂ 97% · Alert & oriented · No complaints
This rhythm strip shows sinus bradycardia. What is the most appropriate action?
- Is this patient hemodynamically stable? Yes
- Does the rate alone require treatment? No
- What is your action? Continue monitoring; document; notify provider if symptomatic
10
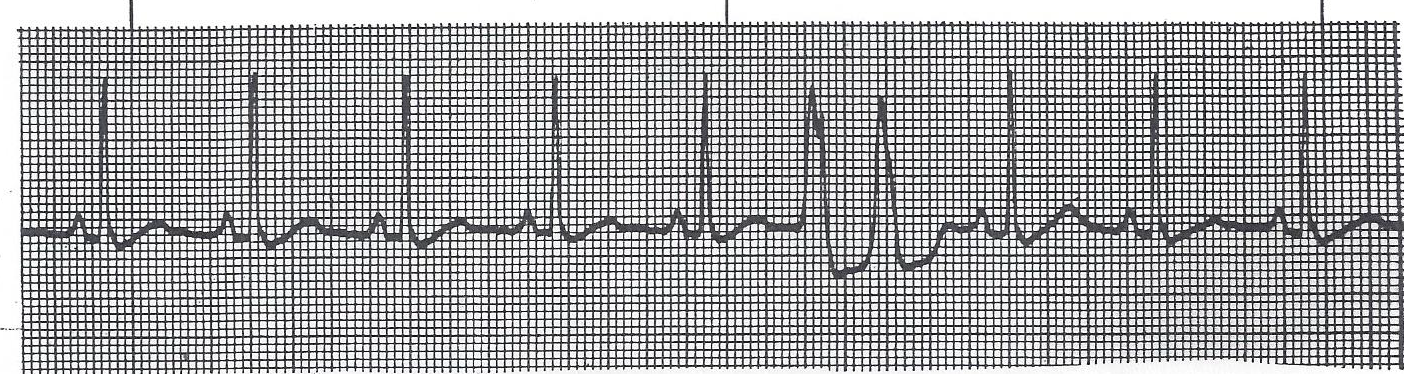
Module 6 · Atrial Rhythms
Rhythm Recognition
PAC (Premature Atrial Contraction)
- Origin: ectopic focus in the atria
- P wave: present but different morphology (abnormal shape)
- Appears earlier than expected
- QRS: usually narrow (narrow / wide)
- Clinical: usually benign / no treatment needed
Atrial Flutter
- Atrial rate: approximately 300 bpm
- Classic pattern: flutter/sawtooth waves (sawtooth)
- Conduction ratio: often 2:1 or 4:1
- Ventricular rate with 4:1 block ≈ 75 bpm
- Risk: can convert to atrial fibrillation
Atrial Fibrillation
- Atrial rate: 350–600 bpm (chaotic)
- Ventricular rhythm: irregularly irregular
- P waves: absent, replaced by fibrillatory (f) waves
- Major risk: thrombus → embolism (stroke)
- Anticoagulation decision: use CHA₂DS₂-VASc score
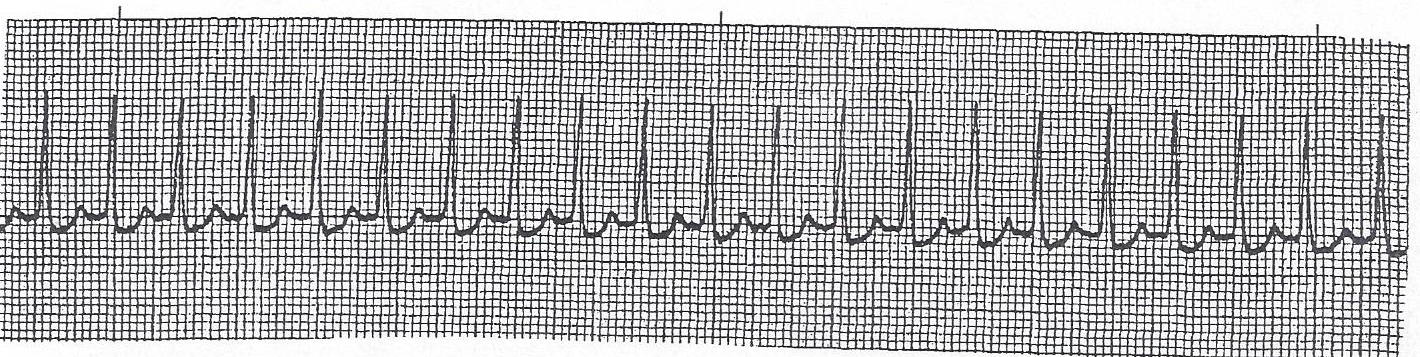
SVT (Supraventricular Tachycardia)
- Rate: 150–250 bpm
- Onset: sudden / gradual (circle one)
- P waves: absent / hidden in QRS or retrograde
- First intervention: vagal maneuver (Valsalva)
- Drug of choice: adenosine (6 mg IV rapid push)
Key Point — AFib
The hallmark of AFib is an irregularly irregular ventricular rhythm with no identifiable P waves.
The big danger isn't the rate — it's the thrombus that forms in the non-contracting atrium.
▶ Practice: Identify the atrial rhythm — P waves present?
Step 5 — QRS / Interpretation
11
Module 7 · Junctional Rhythms
Rhythm Recognition
When the AV Junction Takes Over
- Junctional rhythms occur when the SA node fails or is suppressed
- Junctional escape rate: 40–60 bpm
- Accelerated junctional rate: 60–100 bpm
- Junctional tachycardia rate: > 100 bpm
P Wave Clues in Junctional Rhythm
- P waves may be: (1) before QRS (inverted in II, III, aVF) (before QRS, inverted) or
- (2) buried in QRS (not visible) (buried in QRS, not visible) or
- (3) after QRS (retrograde) (after QRS)
- When P wave precedes QRS, PR interval is shorter than normal (< 0.12 sec)
- QRS width: usually narrow (narrow / wide)
Clinical Significance
| Type | Rate | Priority | Common Cause |
|---|
| Junctional Escape |
40–60 bpm |
Monitor; treat underlying cause |
SA node failure, vagal tone |
| Accelerated Junctional |
60–100 bpm |
Monitor |
Dig toxicity, inferior MI, post-cardiac surgery |
| Junctional Tachycardia |
> 100 bpm |
Urgent — treat |
Dig toxicity, ischemia |
Key Point
Junctional rhythms are escape rhythms — the junction fires because a higher pacemaker failed.
The key question: why did the SA node fail? Look for medications, ischemia, or high vagal tone.
Inverted P wave rule: If P waves are inverted in leads II, III, and aVF → the impulse is going up the atria instead of down → junctional or ventricular origin.
▶ Practice: Where are the P waves?
Step 5 — QRS / Interpretation
12
Independent Practice — Break 2
Atrial & Junctional Rhythms · Complete independently · Review with class after break
Apply the 5-Step Rhythm Method to every strip: Rate → Rhythm → P Waves → PR Interval → QRS Width → Interpretation. Complete independently before the group review.
B2-1
Independent Practice — Break 2 (cont.)
Atrial & Junctional Rhythms · Strips 4–6
B2-2
Independent Practice — Break 2 · Clinical Scenario
Apply: Recognize → Assess → Act
68-year-old female with known chronic AFib on anticoagulation therapy. Current vitals: HR 148, BP 106/72, SpO₂ 96% RA, alert and oriented. Complains of palpitations and mild fatigue.
- What rhythm is shown? _______________________________________________
- What is the rate? ___________________________________________________
- Is this patient stable or unstable based on HR 148, BP 106/72, and mental status? _________________________________________
- What is your FIRST nursing action? _________________________________________
B2-3
Module 8 · Ventricular Rhythms & Arrest
Rhythm Recognition · Emergency
| Rhythm |
QRS Width |
Rate |
Key Feature |
Immediate Action |
| PVC |
> 0.12 sec |
Varies |
Wide, bizarre QRS, no P wave before |
Monitor; treat if >6/min or runs |
| V-Tach (sustained) |
Wide |
> 100 bpm |
≥ 3 consecutive PVCs |
If stable: amiodarone; if unstable: synchronized cardioversion |
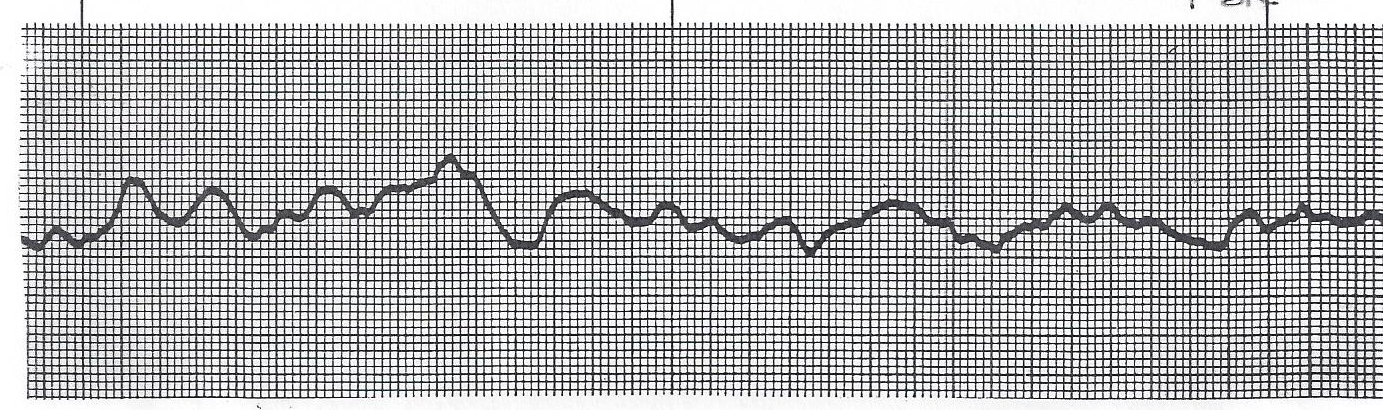
| Ventricular Fib |
No QRS |
No pulse |
Chaotic, no recognizable complexes |
Immediate defibrillation + CPR |
| Idioventricular |
Wide |
20–40 bpm |
Escape rhythm |
Do NOT suppress; find cause |
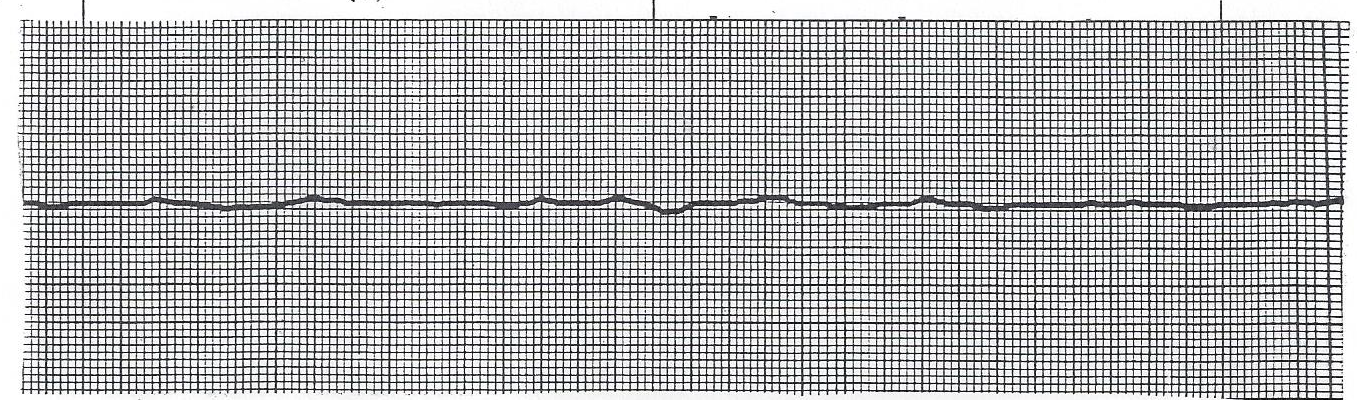
| Asystole |
None |
0 |
Flat line / no electrical activity (flat line) |
CPR, epinephrine, find cause |
PVC Patterns — Know These
- Unifocal PVCs: all look alike (same morphology) (same shape)
- Multifocal PVCs: different shapes / morphologies — more concerning
- Bigeminy: every 2nd beat is a PVC
- Trigeminy: every 3rd beat is a PVC
- Couplet: 2 PVCs in a row
- Triplet: 3 PVCs in a row
- R-on-T phenomenon: PVC falls on the T wave → can trigger ventricular fibrillation
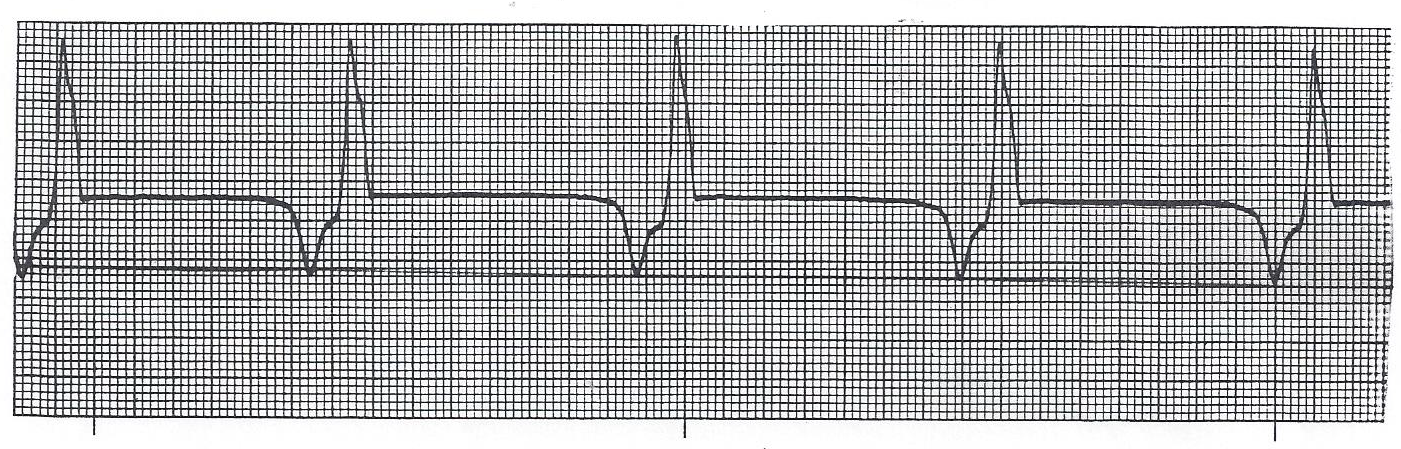
▶ Practice: Wide QRS — count the rate, check for P waves
Step 5 — QRS / Interpretation
⚡ Defibrillation is the only definitive treatment for VFib and pulseless V-Tach.
Begin CPR immediately while the defibrillator charges. Every second counts.
13
Independent Practice — Break 3
Ventricular Rhythms · Complete independently · Review with class after break
Apply the 5-Step Rhythm Method to every strip: Rate → Rhythm → P Waves → PR Interval → QRS Width → Interpretation. Complete independently before the group review.
B3-1
Independent Practice — Break 3 (cont.)
Ventricular Rhythms · Strips 4–6
B3-2
Independent Practice — Break 3 · Clinical Scenario
Apply: Recognize → Assess → Act
Post-operative day 1 patient found unresponsive in bed. Monitor shows wide complex tachycardia at rate 180 bpm. No palpable pulse. Code team has been activated.
- What rhythm is shown? _______________________________________________
- What is the rate? ___________________________________________________
- What did the nurse find when checking for a pulse? _________________________________________
- What is the appropriate treatment pathway for this rhythm without a pulse? _________________________________________
B3-3
Rhythm Identification Flowchart
Bedside Reference Tool
You see a rhythm on the monitor
↓
Is the PR interval present and CONSISTENT?
PR progressively
LENGTHENS → dropped QRS?
Cycle repeats (group patterns)
↳ Wenckebach (Type I)
PR FIXED → sudden
dropped QRS?
No progressive change
↳ Mobitz II (Type II) ⚠
P waves & QRS completely
UNRELATED (diff. rates)?
AV dissociation
↳ 3rd-Degree Block 🚨
PR > 0.20 sec but
ALL beats conduct?
No dropped beats
↳ 1st-Degree Block ✔
↓ If no block pattern identified — continue to 5-Step Method below ↓
1 What is the RATE?
▸ < 60
→ Bradycardia branch
Sinus Brady / Junctional Escape / Idioventricular
▸ 60–100
→ Normal rate
NSR / 1° Block / PAC / PVC
▸ > 100
→ Tachycardia branch
Sinus Tachy / SVT / AFib / VTach
2 Is rhythm REGULAR or IRREGULAR?
▸ Irreg. irreg.
→ Think AFib first
▸ Regularly irreg.
→ Group patterns suggest Wenckebach or PACs
3 Are P WAVES present?
▸ None
→
Junctional or Ventricular origin
▸ Inverted
→
Junctional (retrograde)
▸ Sawtooth
→
Atrial Flutter
▸ Fibrillatory
→
Atrial Fibrillation
▸ Upright × 1
→ Sinus origin likely
4 PR INTERVAL
▸ 0.12–0.20s
Normal — Sinus origin likely
> 0.20s
1st Degree AV Block
▸ < 0.12s
→
Junctional or WPW
▸ Absent / var.
→ Block or Junctional/Ventricular
5 QRS WIDTH
▸ < 0.12s
Narrow → Supraventricular origin
▸ ≥ 0.12s
Wide → Ventricular or aberrant SVT
▸ Paced wide
Look for pacer spikes
Common Terminal Diagnoses
NSR
Sinus Brady
Sinus Tach
1° Block
SVT / PSVT
AFib
AFlutter
Wenckebach
Junctional
PVCs
Mobitz II ⚠
V-Tach
V-Fib 🚨
3° Block 🚨
Idioventricular
Orange = Monitor / Assess patient
Dark Red = Emergency / Immediate intervention
Always: After identifying the rhythm — assess the patient. Rate and rhythm only matter in context. Ask: "Is my patient hemodynamically stable?"
14
Practice Strips
Apply the 5-Step Method · Interpret Each Strip
Apply the 5-Step Rhythm Method to every strip: Rate → Rhythm → P Waves → PR Interval → QRS Width → Interpretation. Complete all fields independently before asking your instructor.
15
Practice Strips (cont.)
Apply the 5-Step Method · Interpret Each Strip
16
Practice Strips (cont.)
Apply the 5-Step Method · Interpret Each Strip
17
Practice Strips (cont.)
Apply the 5-Step Method · Interpret Each Strip
18
Practice Strips (cont.)
Apply the 5-Step Method · Interpret Each Strip
19
Practice Strips (cont.)
Apply the 5-Step Method · Interpret Each Strip
20
Practice Strips (cont.)
Apply the 5-Step Method · Interpret Each Strip
21
Practice Strips (cont.)
Apply the 5-Step Method · Interpret Each Strip
22
Practice Strips (cont.)
Apply the 5-Step Method · Interpret Each Strip
23
Practice Strips (cont.)
Apply the 5-Step Method · Interpret Each Strip
Well done! You've worked through 20 strips using the 5-step method.
Rhythm interpretation is a skill built with repetition. Keep practicing, and always connect the rhythm to your patient's clinical picture.
Remember: Recognize → Assess → Act.
24
Final Assessment · Practice Strips — Capstone
🎓 Recognize → Assess → Act
Instructions — For each strip below, complete all three steps:
- Name the rhythm using your 5-step method (Rate → Rhythm → P Waves → PR Interval → QRS)
- State the stability criteria you would assess at the bedside (mental status, BP, SpO₂, symptoms)
- Describe your first action — what would you do if this patient is stable? If unstable?
Strip A
Stability criteria I would assess
If stable — first action:
If unstable — first action:
Strip B
Stability criteria I would assess
If stable — first action:
If unstable — first action:
Strip C
Stability criteria I would assess
If stable — first action:
If unstable — first action:
25